Beyond Shelter: San Francisco’s Holistic Approach to Caring for the Homeless
March 5, 2019 Dr. Barry Zevin has been working with people who are homeless for the better part of three decades. As the medical director for Street Medicine and Shelter Health Center in San Francisco, he knows well the extraordinary level of care and attention some of those experiencing homelessness need.
Zevin’s outreach team recently encountered a 40-year old man experiencing homelessness who had schizophrenia, as well as methamphetamine and opioid use disorder, and was seeking help for a heroin addiction.
HOW THE CITY IS WORKING TO IMPROVE HEALTH OUTCOMES
Using an integrated data system to show a patient’s health history
Meeting between social service agencies to address patients’ overall needs
Developing shared methods for prioritizing resources
To learn more about the patient, Zevin looked up the man’s profile in the city’s Coordinated Care Management System (CCMS), an integrated data system that allows healthcare providers to see not just their patients’ medical health history, but also their use of mental health services, homeless shelters, housing services, sobering centers, emergency services, public benefits, and more. Zevin discovered that the man had a long history of social service use — and of aggressive behavior that had caused him to be restricted from many city services.
“He would experience psychosis from his schizophrenia or from his methamphetamine use, and he would lash out at other patients and sometimes at staff,” Zevin said. “When we asked what it would take to get him back to treatment, he said, ‘See me outside. I’m fine out here. But if you need to see me inside, I need a quiet place. I can’t deal with the people in the waiting room.’” Zevin and his team invited the man to their open access clinic and gave him a quiet place to wait when he arrived. Soon after, he was receiving treatment for his heroin addiction.
According to the California Department of Health Care Services, these types of complex patients who frequently use urgent and emergent healthcare services make up roughly 5 percent of MediCal (California’s Medicaid program) users. But they account for more than 50 percent of MediCal spending.
Zevin’s deep experience tells him that highly vulnerable patients who are at high risk of death need a completely different model of care. “If you ever want to take care of the patient experiencing schizophrenia who can’t sit in your waiting room, you’re going to have to do something different than what you do now,” he said. “We need to adapt to the needs of this patient.”
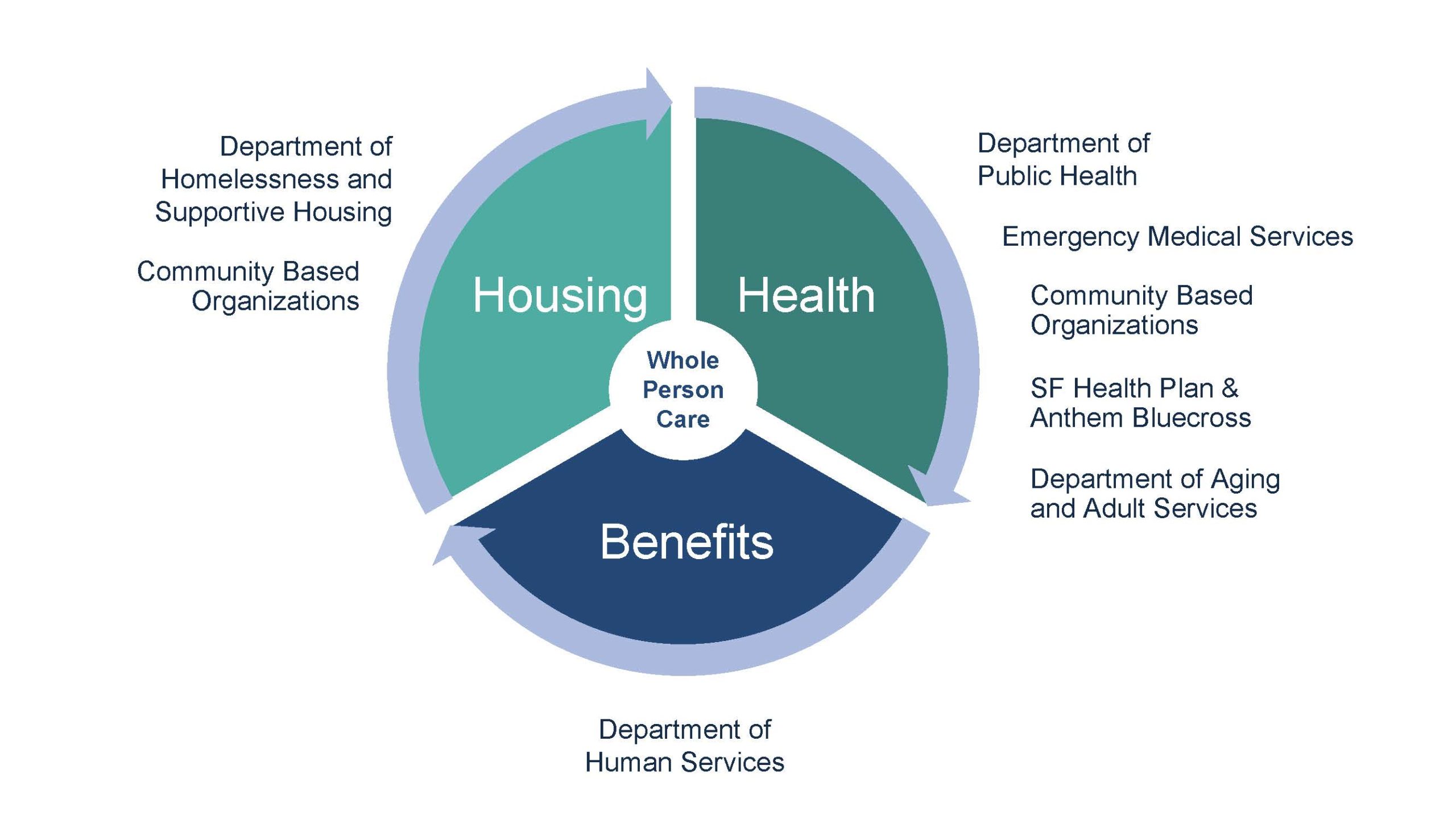
The Whole Person Care program creates an imperative for health, housing, and benefits partners to work together in a human-centered fashion.
Such an innovative approach to healthcare is being tested under California’s Whole Person Care (WPC) pilot program. The program, which rolled out in 2017 and ends in 2020, gives counties and health authorities funding to introduce more coordinated, human-centered models of care for MediCal recipients who are heavy users of health and social services but continue to have poor outcomes.
Since the program’s inception, 25 WPC pilots have been approved, including in Orange, Los Angeles, Alameda, and Napa counties. The City and County of San Francisco’s proposal focused on adults experiencing homelessness and is a partnership among the departments of Public Health (DPH), Homelessness and Supportive Housing (HSH), Aging and Adult Services (DAAS), Human Services (DHS), and the two county health plans. The pilot was expanded in a second round of applications approved by the state in 2017. Street Medicine and Shelter Health is a DPH team that receives funding from the program, which aims to stabilize highly vulnerable, high-risk patients on the street so that they can eventually move into the traditional healthcare system.
Ahead of the Curve
San Francisco has long been a laboratory for a holistic approach to healthcare. For example, when CCMS was introduced in 2005, it was the first integrated data management system of its kind. “We had to start from scratch,” said San Francisco Whole Person Care director Maria X Martinez, who pioneered the effort to pull information from more than a dozen separate data systems across the city into one place. Martinez knew this centralized data would be critical to determining how best to help the city’s most vulnerable residents — especially those experiencing homelessness — gain access to the healthcare and wraparound services they need.
Agency partners work together to serve shared clients and identify opportunities for future improvement. Photo credit: SF DPH
By 2007, CCMS was robust enough that frontline healthcare providers could see diagnostic information as well as which city services were used by the most at-risk patients. The system included any patient who had been homeless, jailed, or engaged in a behavioral health service, or who had used any urgent or emergent service. Once matched and merged into a single record, health histories were available going as far back as 1998.
From this data, providers can see a summary of the whole person and then treat or refer the patient accordingly. Martinez was also able to use CCMS to better understand San Francisco’s most vulnerable populations, those who rely on urgent and emergent services across the medical, psych, and addiction systems of care. These individuals were deemed the highest users of multiple systems, or HUMS. As it turned out, a high proportion of the city’s HUMS also experience homelessness. When it came time to apply for the state’s WPC pilot, San Francisco knew who the target population should be. “Our goal is to assess every single homeless person for their health needs, their housing needs, and their benefits eligibility,” Martinez said, “and also to crack the nut on how to prevent and respond to HUMS.”
To work toward this goal, Martinez collaborates with a steering committee that includes the partner agencies. “Funded positions within each agency have the Whole Person Care mission and vision attached to them,” said Erica Medina Stanulis, a FUSE executive fellow who is working with Martinez to implement the pilot program. “But Whole Person Care is not an actual department, and it doesn’t have any formal authority to enact changes. Any changes that the team brings about have to come through listening to and influencing frontline staff and leadership, breaking down silos, and solving problems together.”
In one example of this cross-departmental collaboration, staff from DHS now travel to two of the city’s largest homeless shelters to share information about available benefits and to assess participants’ eligibility for public benefits. They also attend weekly shelter staff meetings. “It’s part of getting on the radar of our colleagues in other departments and vice versa,” said Susie Smith, deputy director of policy and planning for the Human Services Agency (the umbrella agency over DHS, DAAS, and the Office of Early Care and Education). “We need to think more holistically about the needs of our shared clients, and how we enable all three services — health, housing, and benefits — to come to clients in the best, most effective, easy-to-access way possible.”
“We need to think more holistically about the needs of our shared clients, and how we enable all three services — health, housing, and benefits — to come to clients in the best, most effective, easy-to-access way possible.” — Susie Smith, deputy director of policy and planning, Human Services Agency
WPC is also developing a shared methodology to prioritize patients who use multiple systems of care and flex existing systems in order to better serve the city’s most vulnerable residents. This methodology will help prioritize clients into scarce resources, such as permanent supportive housing, residential care, care planning and stabilization, and more. Currently, each agency and service has its own way of prioritizing the highest need patients. Zevin gives an example of a patient who requires residential treatment for co-occurring mental-health and substance-abuse disorders. “I say, ‘My guy needs this, and he’s ready today.’ And the person who has control of those slots says, ‘We’ve got a slot, but, sorry, it’s reserved for somebody who meets this other profile that our individual system has determined is higher priority,’” Zevin said. “I’m upset, because even though my guy was ready and needed it, he didn’t get it because somebody else’s priority came first.”
The committee is developing a process that will determine a shared methodology of how priority clients are identified and create a shared governance and response system among health, housing, and benefits. Other challenges being addressed include getting and keeping homeless adults on MediCal, training staff to think beyond their respective silos, and ensuring that the WPC approach is sustained beyond 2020, when state funding for the program is slated to end. By then, the city expects to have the infrastructure, technology, and protocols for information sharing and accountable care coordination fully in place so it can continue with its WPC program.
Three key components
For the WPC approach to become sustainable, however, a few crucial ingredients must come together. “One is leadership,” said Martinez, “and that happens at two levels. The people at the very top have to say, ‘Yes, I sanction this, and I will carve out my attention and my priorities to support it.’ The other kind of leadership is making sure someone sees it through and just does it.” Martinez shares the latter role with leaders in her sister agency partners.
The agencies also need to determine how to share patient information without running afoul of privacy laws and ethics. “You have to have your lawyers and your privacy people and your legislators create language that allows and protects the sharing of sensitive information. ‘Need to know’ and ‘minimum necessary’ should be our guiding faculty once that authority is obtained,” Martinez said.
Finally, the technology has to be in place to enable the kind of data sharing that makes coordinated care possible on the patient level, assures appropriate role-based access, and improves the management on a caseload level. It has to make jobs easier, not more complicated. “Those three things — leadership, privacy, and technology — have to align with the funding to make it happen,” said Martinez.
The results of taking a Whole Person Care approach with patients, such as the homeless man Zevin’s team encountered on the streets of San Francisco, can be transformational. “He’s incredibly stabilized compared to where he was,” said Zevin.
Once incapable of sitting in a waiting room without fleeing or flying into a rage, the man has gradually progressed in his treatment. So when he developed a serious infection in his legs, he was able to transition from Street Medicine to a local respite center to recover. “It’s a dormitory style program. One bed is right next to the next to the next,” Zevin said. “This was something that would have been unimaginable for this patient before.” Now, Zevin said, he’s on the cusp of being housed.
Rikha Sharma Rani is a Bay-area based writer and journalist. Her work has been featured in The New York Times, USA Today, Politico Magazine, CityLab, and more.[Photo credit: Ev]